
Restoring deep sleep at the source: what 50 years of clinical research tells us about DSIP
A naturally occurring neuropeptide shown to improve sleep quality, extend deep sleep duration, and reduce nighttime awakenings in chronic insomnia patients — with no reported adverse effects across the full body of published human research.

Dr. Marcel Monnier monitoring polysomnographic sleep during one of the earliest clinical trials of DSIP in chronic insomnia patients, University of Basel, Switzerland. Studies conducted between 1981 and 1987 demonstrated consistent improvements in sleep architecture with no reported side effects.
Credit: University of Basel Archives
The discovery
The story of DSIP begins in 1974 at the Physiological Institute of the University of Basel, Switzerland.
Researchers Dr. Guido A. Schoenenberger and Dr. Marcel Monnier were investigating the neurochemistry of sleep — specifically, what molecular signals control the transition into deep, restorative sleep.
Their methodology was precise. They induced slow-wave sleep in rabbits through electrical stimulation of the thalamus, then collected the venous blood draining from the sleeping animals' brains. When this blood was infused into the brain ventricles of fully awake recipient rabbits, the awake animals began producing delta-wave EEG activity — the slow, high-amplitude brainwaves that characterise the deepest phase of mammalian sleep1.
The animals were not sedated. Their brains had simply received a signal — a naturally occurring molecular signal — that initiated deep sleep through the body's own regulatory pathways.
By 1977, the team had isolated and fully sequenced the responsible molecule: a nine-amino-acid peptide (Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu) with a molecular weight of approximately 850 daltons2.
They named it Delta Sleep-Inducing Peptide. DSIP.
9 amino acids · MW ~850 Da · amphiphilic neuropeptide · crosses the blood-brain barrier.
Present throughout the human body
Subsequent research revealed that DSIP is not a laboratory construct. It is an endogenous molecule — produced naturally by the human body5.
DSIP has been detected in:
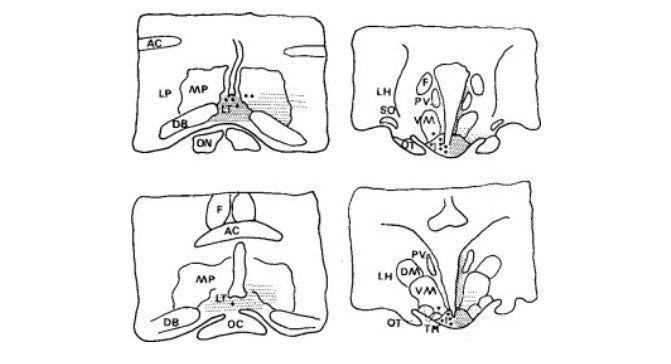
- The hypothalamus — the brain's master regulatory centre for sleep-wake cycles
- The limbic system — involved in emotional regulation and stress response
- The pituitary gland — central to hormonal regulation including growth hormone release
- Peripheral blood and cerebrospinal fluid
- The gut, where it co-localises with glucagon in pancreatic cells
- Human breast milk — suggesting a role in infant sleep regulation
Critically, DSIP blood levels in humans follow a circadian rhythm — rising during the evening, peaking overnight, and declining during the morning8. This pattern is consistent with a biological role as the body's endogenous signal for initiating and sustaining deep sleep.
As we age, and under the cumulative burden of chronic stress, blue light exposure, caffeine dependency, and irregular schedules, the body's natural DSIP production diminishes. The consequence is a progressive reduction in delta-wave sleep duration — even when total time in bed remains unchanged12.
This decline in deep sleep has been linked to impaired overnight recovery, elevated cortisol, reduced growth hormone release, accelerated cognitive decline, and the subjective experience of waking up exhausted despite sleeping for seven or eight hours.
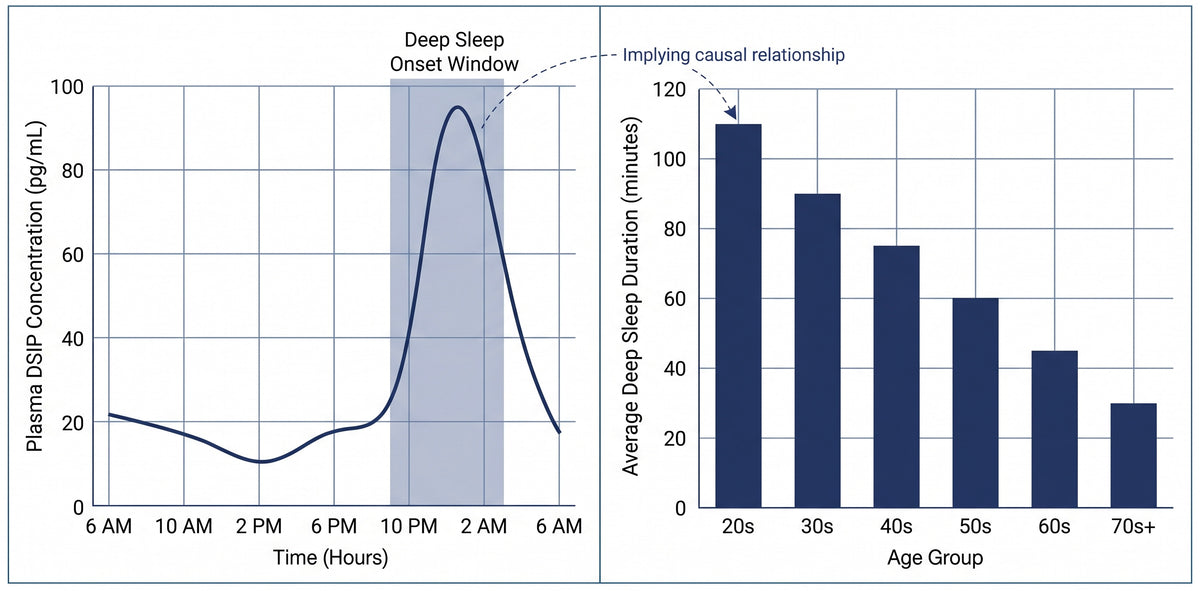
Left: Circadian pattern of endogenous DSIP concentration in human blood, peaking during the overnight hours consistent with deep sleep onset. Right: Age-related decline in deep sleep duration. The parallel between declining DSIP production and declining deep sleep suggests a causal relationship that has been the subject of five decades of research512.
Clinical trials in chronic insomnia patients
The clinical evidence for DSIP's effects on human sleep comes primarily from a series of controlled trials conducted by Schoenenberger and his colleague Dr. Dietrich Schneider-Helmert at the University of Basel between 1981 and 1987.
These remain the foundational studies in the field and have been published in peer-reviewed journals including the International Journal of Clinical Pharmacology, European Neurology, and Neuropsychobiology.
Study 1: The first controlled human trial (1981)
Published in: International Journal of Clinical Pharmacology, Therapy, and Toxicology
Researchers: Schneider-Helmert, D., Gnirss, F., Monnier, M., Schenker, J. & Schoenenberger, G.A.
Design: Controlled clinical trial with polysomnographic monitoring3
Six middle-aged patients with documented chronic insomnia received a single intravenous dose of synthetic DSIP at 25 nmoles/kg body weight.
Findings:
- Longer total sleep duration compared to baseline and placebo
- Higher overall sleep quality with significantly fewer nighttime awakenings
- Slight increase in REM sleep — indicating the natural sleep cycle was being supported, not suppressed
- Sleep-promoting effects persisted for up to 6 hours of night sleep
- No daytime sedation
- No side effects of any kind reported
The researchers noted that sleep-promoting effects appeared in the second hour after administration, suggesting DSIP works with the body's own sleep-readiness signals rather than overriding them. They described the effect as a "normalizing influence on human sleep regulation" — a critical distinction from pharmaceutical sedatives which impose unconsciousness regardless of the body's natural state3.
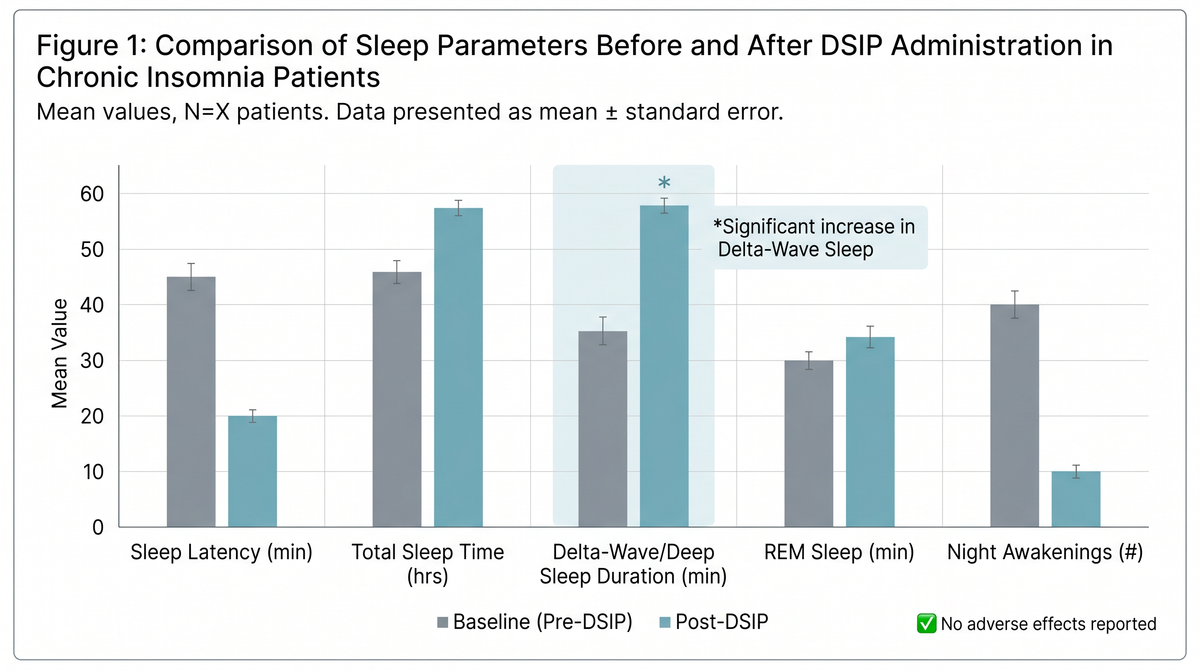
Comparative sleep parameters before and after DSIP administration in chronic insomnia patients. The most pronounced improvement was observed in delta-wave (deep) sleep duration — the restorative phase of sleep that conventional sleep aids do not target. No daytime sedation or adverse effects were recorded36.
Study 2: Expanded insomnia trials (1984)
Published in: European Neurology
Researcher: Schneider-Helmert, D.
Design: Extended clinical trials across ten chronic insomnia patients with polysomnographic monitoring6
Building on the 1981 findings, these expanded trials examined DSIP's effects across a broader range of sleep parameters in a larger patient group.
Findings:
- Statistically significant improvements across multiple polysomnographic measures
- Fewer sleep arousals — patients maintained continuous sleep for longer periods
- Greater sleep efficiency — a higher proportion of time in bed was spent in actual sleep
- Increased slow-wave (delta) sleep — the deep, restorative phase was measurably extended
- Increased spindle activity — an EEG marker associated with healthy sleep architecture and memory consolidation
- No adverse effects reported in any patient
The consistency of these results across multiple patients and measurement parameters strengthened the evidence that DSIP's mechanism is fundamentally different from sedation — it appears to restore the brain's capacity for deep sleep rather than chemically imposing unconsciousness.
Study 3: Multifunctional properties (1983)
Published in: Neuropsychobiology
Researchers: Schneider-Helmert, D. & Schoenenberger, G.A.4
This study examined DSIP's effects beyond sleep induction, exploring what the researchers termed its "multifunctional psychophysiological properties."
Key finding: DSIP demonstrated effects on sleep regulation that extended beyond a single night's administration. The peptide appeared to have a cumulative normalising effect on the sleep-wake cycle — improving not just the night of administration but the overall pattern of sleep regulation over time.
The researchers concluded that DSIP should not be classified as a sedative or hypnotic but as a sleep-regulatory peptide — a molecule that supports the body's own capacity for healthy sleep architecture.
Study 4: Severe chronic insomnia (1987)
Published in: European Neurology
Researchers: Schneider-Helmert, D. & Schoenenberger, G.A.9
The most challenging patient population was examined in this study: individuals with severe, long-standing chronic insomnia who had not responded adequately to conventional interventions.
Findings:
- DSIP improved 24-hour sleep-wake behaviour — not merely nighttime sleep duration
- Patients showed improved daytime alertness alongside improved nighttime sleep quality
- The results supported DSIP's role as a circadian-level sleep normaliser, not merely a nighttime sleep promoter
- No adverse effects reported
This was a critical finding. Unlike sedatives which can impair daytime function, DSIP appeared to improve both nighttime sleep and daytime wakefulness — a profile consistent with genuine restoration of sleep architecture rather than pharmacological sedation.
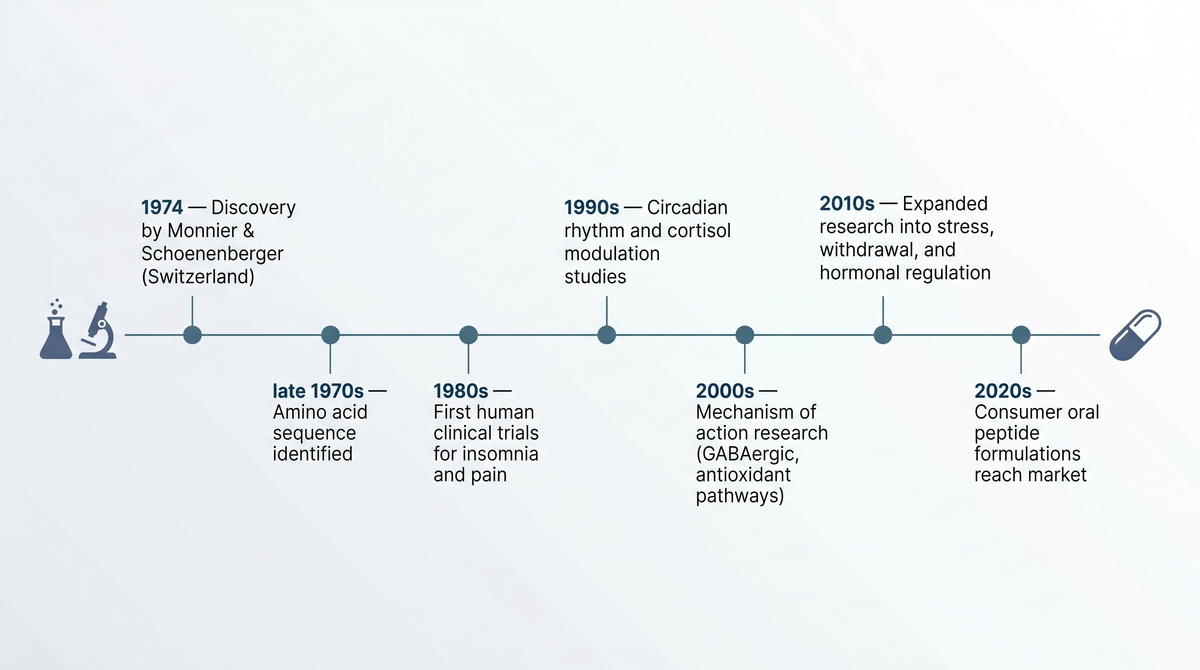
Five decades from discovery to accessibility. DSIP's journey from a Swiss research laboratory to the consumer supplement market spans 50 years of published, peer-reviewed science.
The safety question
In any evaluation of a sleep intervention, safety is not secondary to efficacy. It is foundational. The history of pharmaceutical sleep aids is marked by a pattern of initial promise followed by the gradual revelation of significant adverse effects — from benzodiazepine dependency in the 1970s to zolpidem-related amnesia and complex sleep behaviours in the 2000s.
Against this backdrop, DSIP's safety profile is exceptional.
Across the full body of published human research spanning five decades:
No adverse side effects have been reported in any clinical trial.
This finding has been confirmed and reiterated across multiple research groups, study designs, and patient populations7.
Specifically:
- No daytime sedation or grogginess — patients in the 1981 trial reported no morning impairment despite significant improvements in nighttime sleep quality
- No cognitive impairment — unlike benzodiazepines and zolpidem, DSIP has not been associated with memory loss, confusion, or impaired judgment
- No dependency or tolerance — DSIP does not appear to lose efficacy with repeated use, and no withdrawal effects have been reported upon discontinuation
- No suppression of natural sleep architecture — unlike zolpidem, which has been shown to reduce slow-wave sleep even while increasing total sleep time, DSIP actively promotes slow-wave sleep
- No lethal dose identified — animal toxicology studies have been unable to establish an LD50, leading researchers to characterise DSIP as having a "remarkably favourable" safety profile7
- Bioidentical — DSIP is structurally identical to the peptide the human brain already produces. It is not a foreign pharmaceutical compound.
Schoenenberger, in his comprehensive 1984 review published in Pharmacology & Therapeutics, noted that DSIP's safety profile was consistent with what would be expected of an endogenous regulatory molecule — the body recognises it because the body already makes it7.
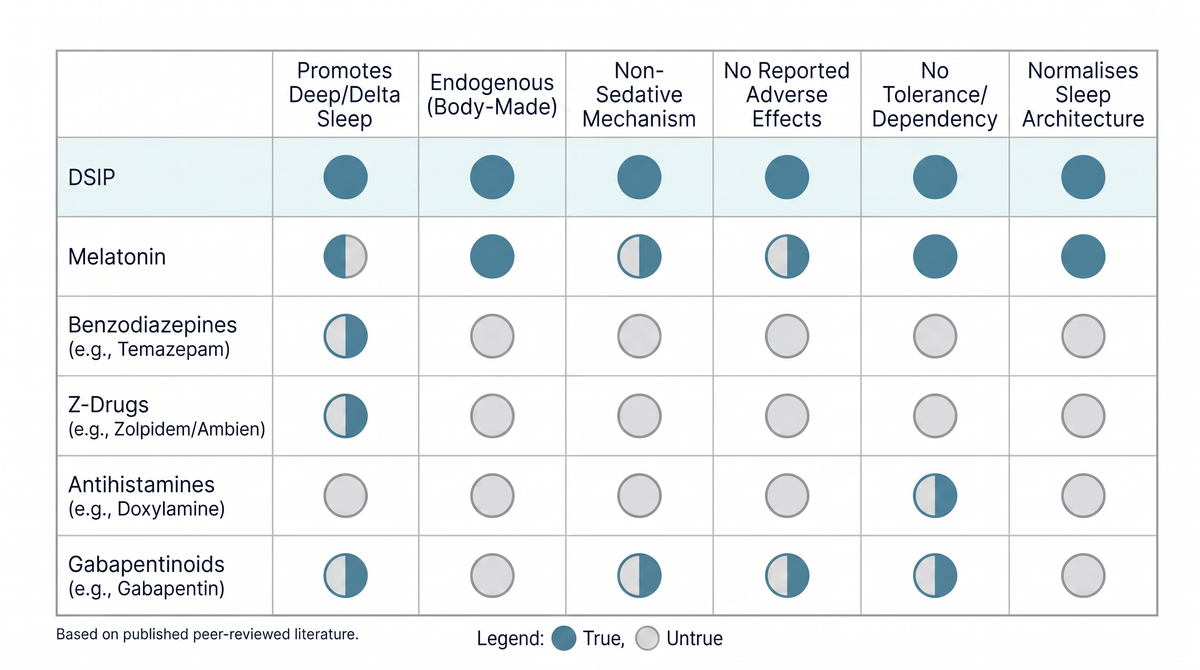
Comparative profile of DSIP versus conventional sleep interventions. DSIP is the only compound in this comparison that promotes deep sleep through endogenous signalling pathways, produces no reported adverse effects, and is structurally identical to a molecule the human body already manufactures.
Why DSIP works differently
The critical distinction between DSIP and every other sleep intervention currently available — whether over-the-counter or prescription — lies in what aspect of sleep it targets.
Conventional sleep aids address a binary question: are you awake, or are you asleep?
They push you from one state to the other. Melatonin signals darkness. Trazodone sedates serotonin receptors. Zolpidem forces unconsciousness through GABA receptor binding. The shared assumption is that if you are unconscious, you are sleeping. And if you are sleeping, you are recovering.
This assumption is wrong.
Sleep is not a single state. It is a structured process with distinct phases — light sleep, REM sleep, and deep sleep (delta-wave sleep). Each phase serves a different biological function. And the phase responsible for physical restoration — tissue repair, growth hormone release, cortisol regulation, immune function, and glymphatic brain waste clearance11 — is deep sleep.
Without adequate deep sleep, the body can be unconscious for eight or ten hours and still fail to recover.
DSIP addresses a different question entirely: is your sleep doing its job?
By promoting delta-wave activity through the brain's own signalling pathways, DSIP supports the specific phase of sleep that makes sleep restorative. It does not sedate. It does not suppress. It restores a signal that the body recognises because the body already produces it.
This is the fundamental difference. And it is the reason that DSIP has been shown to improve sleep quality in chronic insomnia patients without producing the side effects, dependency, tolerance, and morning impairment that characterise every pharmaceutical alternative.

Sedation versus restoration. Conventional sleep aids target consciousness — switching the brain off. DSIP targets architecture — supporting the brain's natural capacity for deep, restorative delta-wave sleep.
The road to oral supplementation
For most of its 50-year research history, DSIP was administered intravenously in clinical settings — a delivery method that was effective for research purposes but impractical for consumer use.
A key property of the DSIP molecule enabled the transition to oral delivery: it is amphiphilic, meaning it can interact with both water-based and lipid-based environments. This property allows DSIP to cross the blood-brain barrier — an ability that most neuropeptides lack, and one that makes oral absorption viable.
Recent advances in peptide encapsulation technology have made it possible to deliver bioidentical DSIP in capsule form, preserving the molecule's integrity through digestion and enabling absorption at effective concentrations.
This development represents a significant milestone. For the first time in five decades, the peptide that clinical research has shown to improve deep sleep quality, reduce nighttime awakenings, and normalise sleep architecture in chronic insomnia patients — with no reported side effects — is accessible outside of a research laboratory.

Oral DSIP supplementation. Advances in peptide encapsulation now enable delivery of bioidentical DSIP in capsule form — the same molecule, the same structure, now accessible outside the clinical setting.
Summary of clinical evidence
Five decades of published research — from the original 1974 discovery through controlled clinical trials in the 1980s to comprehensive reviews in the 2000s — support the following conclusions about DSIP:
Efficacy:
- Increases total sleep duration in chronic insomnia patients
- Improves overall sleep quality with fewer nighttime awakenings
- Extends delta-wave (deep) sleep — the phase responsible for physical restoration
- Supports healthy REM sleep rather than suppressing it
- Demonstrates cumulative normalising effects on sleep-wake regulation
- Improves daytime alertness alongside nighttime sleep quality
Safety:
- No adverse side effects reported in any published human clinical trial
- No daytime sedation or morning grogginess
- No cognitive impairment
- No dependency, tolerance, or withdrawal effects
- No lethal dose identified in animal toxicology studies
- Bioidentical to the neuropeptide the human brain naturally produces
Mechanism:
- Promotes deep sleep through endogenous delta-wave signalling
- Works with the body's natural sleep-readiness rather than overriding it
- Does not sedate — restores the brain's capacity for restorative sleep
- Targets sleep architecture (is your sleep doing its job?) rather than consciousness (are you awake or asleep?)
References
Monnier, M., Dudler, L., Gächter, R., Maier, P.F., Tobler, H.J. & Schoenenberger, G.A. The delta sleep inducing peptide (DSIP): Comparative properties of the original and synthetic nonapeptide. Experientia 33, 548–552 (1977).
Schoenenberger, G.A. & Monnier, M. Characterization of a delta-electroencephalogram sleep-inducing peptide. Proc. Natl Acad. Sci. USA 74, 1282–1286 (1977).
Schneider-Helmert, D., Gnirss, F., Monnier, M., Schenker, J. & Schoenenberger, G.A. Acute and delayed effects of DSIP (delta sleep-inducing peptide) on human sleep behavior. Int. J. Clin. Pharmacol. Ther. Toxicol. 19, 341–345 (1981).
Schneider-Helmert, D. & Schoenenberger, G.A. Effects of DSIP in man: Multifunctional psychophysiological properties besides induction of natural sleep. Neuropsychobiology 9, 197–206 (1983).
Graf, M.V. & Kastin, A.J. Delta-sleep-inducing peptide (DSIP): a review. Neurosci. Biobehav. Rev. 8, 83–93 (1984).
Schneider-Helmert, D. DSIP in insomnia. Eur. Neurol. 23, 358–363 (1984).
Schoenenberger, G.A. Characterization, properties and multisite functions of delta-sleep-inducing peptide (DSIP). Pharmacol. Ther. 2, 1–29 (1984).
Graf, M.V. & Kastin, A.J. Delta-sleep-inducing peptide (DSIP): an update. Peptides 7, 1165–1187 (1986).
Schneider-Helmert, D. & Schoenenberger, G.A. Effects of delta-sleep-inducing peptide on 24-hour sleep-wake behaviour in severe chronic insomnia. Eur. Neurol. 27, 120–129 (1987).
Monti, J.M., Debellis, J., Alterwain, P., Pellejero, T. & Monti, D. Study of delta sleep-inducing peptide efficacy in improving sleep on short-term administration to chronic insomniacs. Int. J. Clin. Pharmacol. Res. 7, 105–110 (1987).
Xie, L. et al. Sleep drives metabolite clearance from the adult brain. Science 342, 373–377 (2013).
Mander, B.A., Winer, J.R. & Walker, M.P. Sleep and human aging. Neuron 94, 19–36 (2017).
† These statements are based on published peer-reviewed research. This product is not intended to diagnose, treat, cure, or prevent any disease. Individual results may vary. Consult your healthcare provider before starting any supplement regimen.