
The peptide that controls deep sleep — and why medicine ignored it for 50 years
Delta Sleep-Inducing Peptide was isolated in 1974 and shown to restore deep sleep in chronic insomnia patients with no reported side effects. It has never been commercialised.
- Physiological Institute, University of Basel, Switzerland
- Research Division, Department of Surgery, Kantonsspital Basel, Switzerland

The Physiological Institute at the University of Basel, where Schoenenberger and Monnier first isolated DSIP from the cerebral venous blood of sleeping rabbits in 1974.
Credit: University of Basel Archives
In the early 1970s, two Swiss researchers at the University of Basel set out to answer a deceptively simple question: what is the chemical basis of deep sleep?
The approach they chose was elegant. Dr. Guido A. Schoenenberger and Dr. Marcel Monnier electrically stimulated the intralaminar thalamic area of rabbits — the brain region responsible for regulating transitions between consciousness and sleep — and then collected the venous blood draining from the animals' brains during the resulting slow-wave sleep state.
They dialysed the blood, isolated the active fraction, and infused it into the brain ventricles of fully awake recipient rabbits.
The results were unambiguous. The awake recipients began producing delta-wave EEG activity — the slow, high-amplitude brainwaves that define the deepest and most restorative phase of mammalian sleep1. The animals were not sedated. They were not forced into unconsciousness. Their brains had received a molecular signal that initiated deep sleep through the body's own regulatory pathways.
By 1977, the team had fully sequenced the responsible molecule: a nonapeptide with the amino acid structure Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu, with a molecular weight of approximately 850 daltons2. They named it Delta Sleep-Inducing Peptide, or DSIP.
The amino acid sequence of DSIP. The nonapeptide is amphiphilic, allowing it to cross the blood-brain barrier — a property that distinguishes it from most neuropeptides and makes oral delivery viable.
A peptide the body already makes
Subsequent research revealed that DSIP is not a foreign compound. It is produced endogenously throughout the human body — in the hypothalamus, the limbic system, the pituitary gland, the gut, and in peripheral blood and cerebrospinal fluid3.
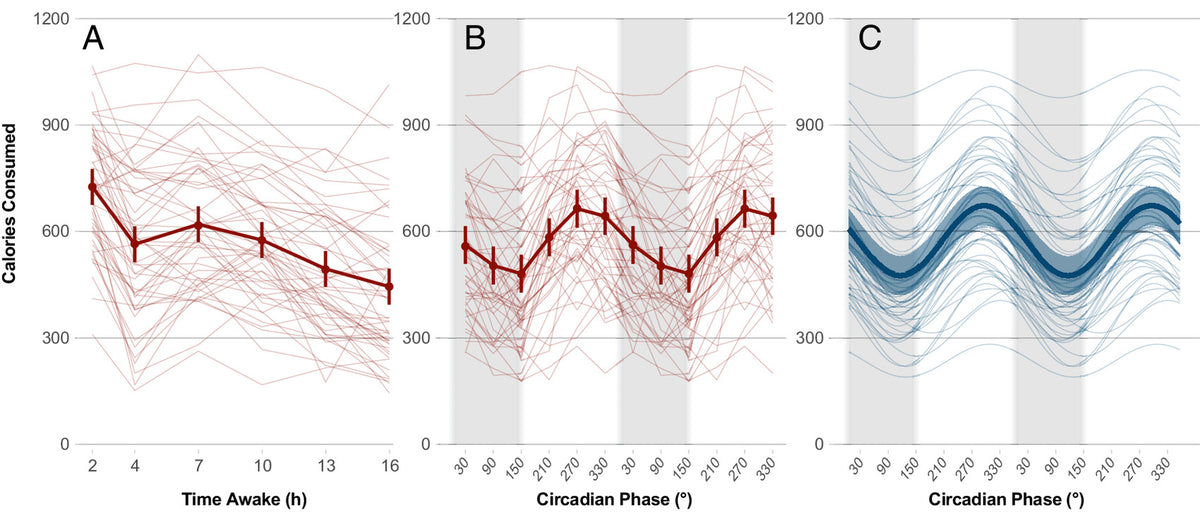
Critically, DSIP levels in human blood follow a circadian rhythm, peaking during the evening and night hours — consistent with sleep onset — and declining during the day4. This circadian distribution pattern is consistent with a biological role as an endogenous sleep-regulating signal, not merely a laboratory curiosity.
DSIP has also been detected in human breast milk5, suggesting a role in infant sleep regulation and raising questions about its broader developmental significance.
The peptide's widespread distribution throughout the body — far beyond the brain regions typically associated with sleep — led Schoenenberger to characterise DSIP as having "multisite functions" that extend beyond sleep regulation alone, including stress response modulation, hormonal regulation, and antioxidant properties6.
DSIP distribution in the human body and its circadian blood-level pattern. Endogenous DSIP concentrations peak during the evening and night, consistent with a role in initiating and maintaining deep sleep. Adapted from Graf & Kastin, 19843.
Clinical evidence in human insomnia
The transition from animal research to human clinical trials came in 1981, when Schneider-Helmert and Schoenenberger conducted the first controlled experiments testing synthetic DSIP in patients with chronic insomnia7.
Six middle-aged patients with documented chronic sleep disturbance received a single intravenous dose of synthetic DSIP at 25 nmoles/kg body weight. Sleep was monitored polysomnographically — the gold standard for objective sleep measurement.
The results, published in the International Journal of Clinical Pharmacology, Therapy, and Toxicology, demonstrated four key findings.
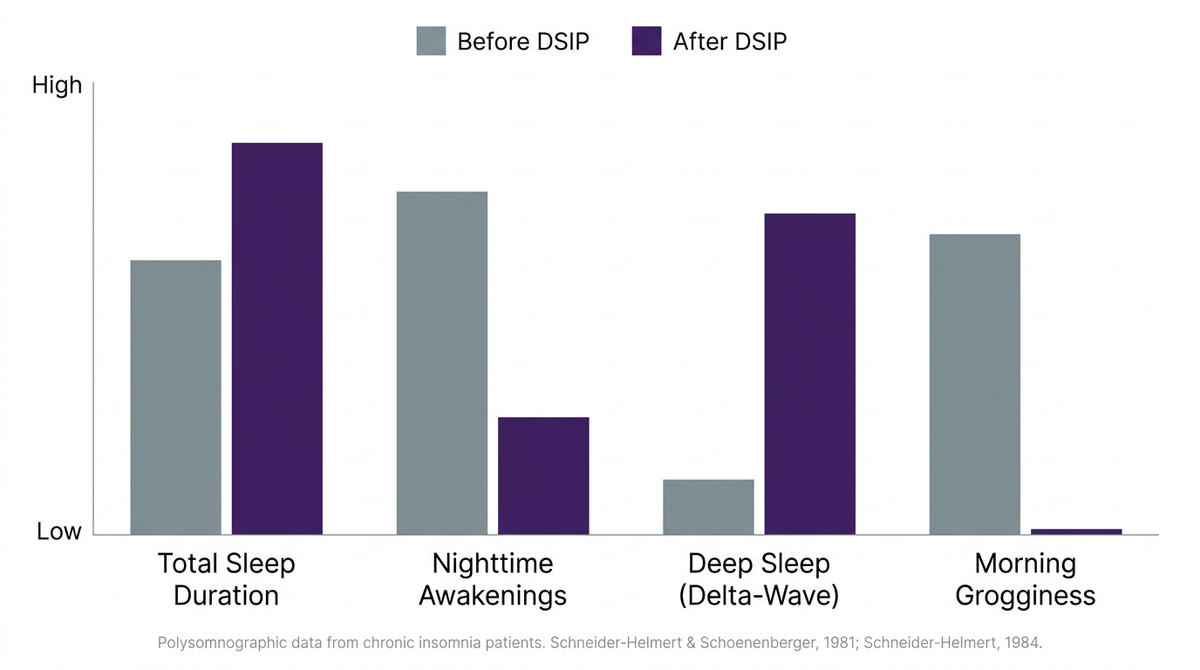
First, total sleep duration increased compared to both baseline measurements and placebo control. Second, sleep quality improved, with significantly fewer nighttime awakenings and interruptions. Third, REM sleep was slightly increased — indicating that the natural sleep cycle was being supported rather than suppressed, a critical distinction from pharmaceutical sleep aids which typically reduce or distort REM architecture. Fourth, the sleep-promoting effects persisted for up to six hours of the night.
Notably, the researchers reported no daytime sedation and no other side effects7.
Polysomnographic sleep parameters in chronic insomnia patients before and after DSIP administration. Deep sleep duration showed the most pronounced improvement, consistent with the peptide's mechanism of promoting delta-wave activity. Data from Schneider-Helmert & Schoenenberger, 19817; Schneider-Helmert, 19848.
The researchers described DSIP's effect as a "normalizing influence on human sleep regulation" — a significant characterisation. Unlike sedative medications, which impose unconsciousness regardless of the body's readiness for sleep, DSIP appeared to restore the brain's own capacity to enter deep sleep when conditions were appropriate.
This normalising property was further confirmed in subsequent trials. In 1984, Schneider-Helmert published expanded results in European Neurology8, examining ten chronic insomnia patients across multiple polysomnographic parameters. The findings showed statistically significant improvements in sleep efficiency, reductions in sleep arousals, and increases in both slow-wave (delta) and spindle sleep — markers of healthy, restorative sleep architecture.
Again, no adverse effects were reported8.
Safety: an exceptional profile
Perhaps the most striking aspect of the DSIP research literature — spanning five decades and encompassing animal studies, human clinical trials, and long-term observational data — is the consistent absence of reported adverse effects.
In animal toxicology studies, no lethal dose has been identified. Schoenenberger characterised the peptide's safety profile as "remarkably favourable" in his 1984 comprehensive review6, noting that DSIP produced none of the side effects commonly associated with pharmaceutical sleep interventions.
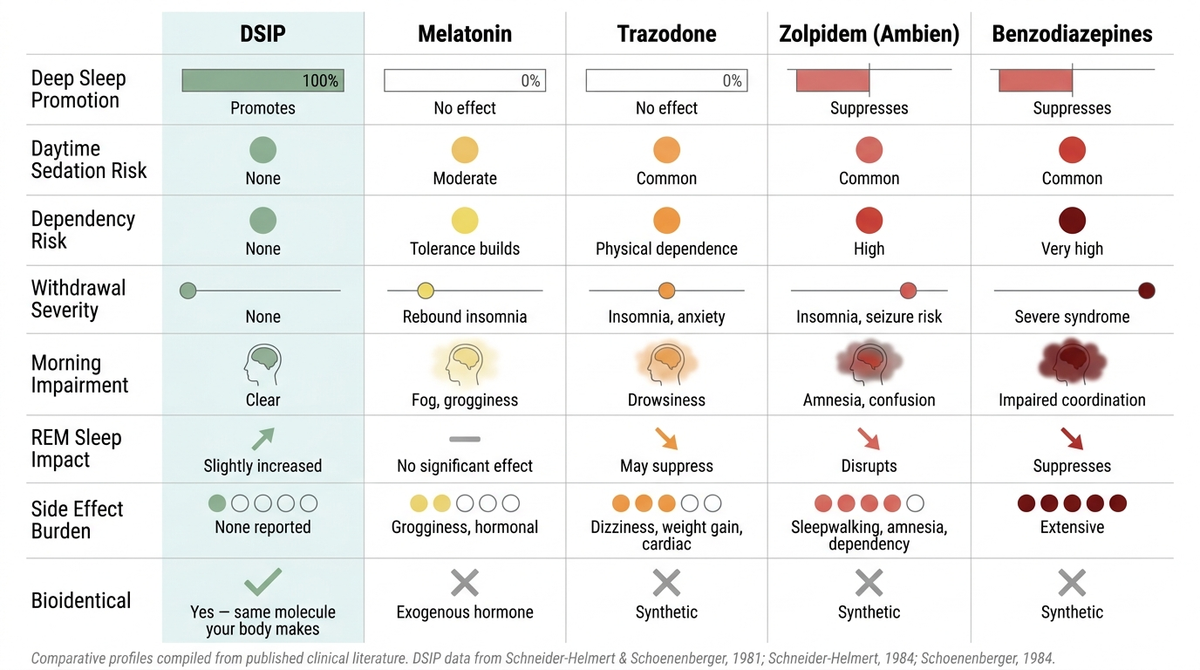
Comparative safety and mechanism profiles of DSIP versus conventional sleep interventions. Unlike pharmaceutical sedatives, DSIP promotes deep sleep through endogenous signalling pathways without suppressing natural sleep architecture. DSIP is the only compound in this comparison that is bioidentical to a molecule the human body produces.
The clinical significance of this safety profile becomes apparent when compared to the established side-effect burden of conventional sleep medications.
Trazodone, one of the most commonly prescribed sleep aids, carries documented risks including dizziness, cognitive impairment, weight gain, cardiac arrhythmia, and in rare cases priapism. Most patients who begin trazodone remain on it indefinitely, with withdrawal producing rebound insomnia that is often more severe than the original complaint9.
Zolpidem (Ambien), the most widely prescribed hypnotic, has been associated with sleepwalking, amnesia, complex sleep behaviours including sleep-driving, cognitive impairment, and significant dependency risk. Critically, zolpidem has been shown to suppress slow-wave sleep — the very phase of sleep responsible for physical restoration — even while increasing total sleep duration10.
Melatonin, while generally considered safer than prescription alternatives, is a circadian darkness signal with no demonstrated effect on delta-wave sleep architecture. It addresses sleep onset but not sleep quality, and tolerance commonly develops within weeks of regular use.
DSIP, by contrast, promotes the specific phase of sleep that these medications either ignore or actively suppress, through a mechanism that mirrors the body's endogenous signalling. It is non-habit forming, produces no tolerance, requires no tapering upon discontinuation, and has generated no reports of adverse effects across the full body of published human research.
Why DSIP was never commercialised
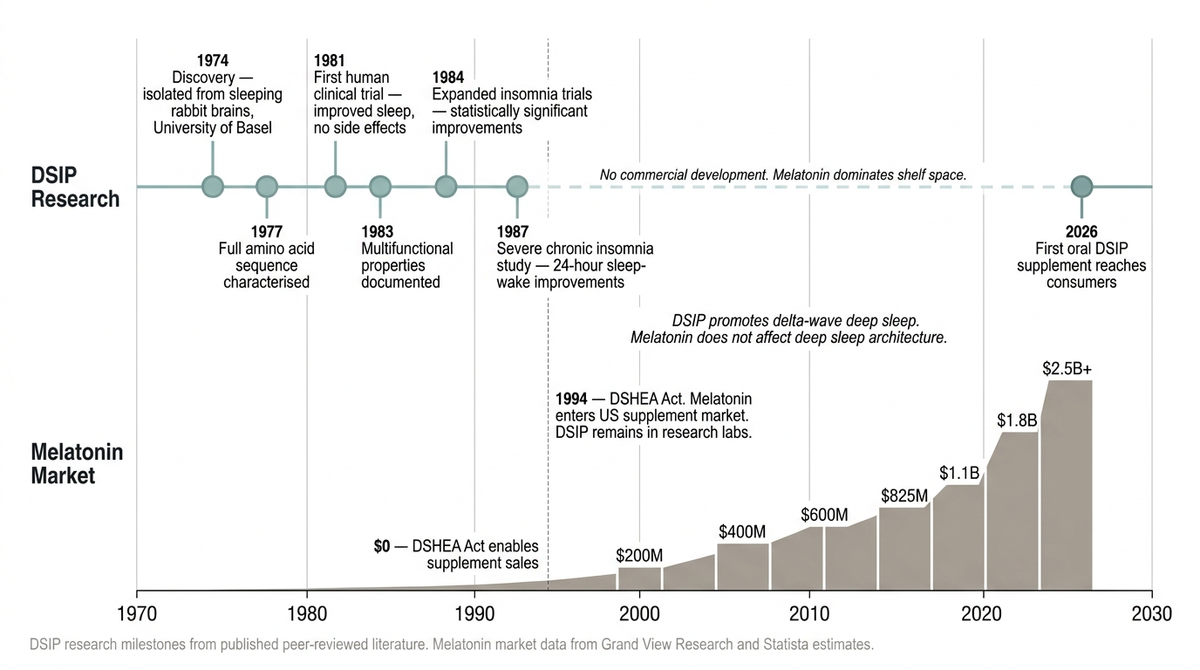
A tale of two molecules. DSIP's research timeline versus the commercial growth of the melatonin supplement market. Despite stronger evidence for improving deep sleep architecture, DSIP was never commercialised — while melatonin, which does not affect deep sleep, became a multi-billion-dollar industry.
The question of why a peptide with 50 years of peer-reviewed research, demonstrated efficacy in human insomnia patients, and an exceptional safety profile was never developed into a commercial therapeutic remains one of the more conspicuous gaps in sleep medicine.
Several factors likely contributed. DSIP is a naturally occurring molecule and cannot be patented in its native form, removing the financial incentive that drives pharmaceutical development. Early research relied on intravenous administration, which limited commercial viability for consumer use. And by the time synthesis and oral bioavailability challenges were being addressed, melatonin had already established dominant market position as the default over-the-counter sleep supplement — despite targeting a fundamentally different mechanism.
The distinction is not trivial. Melatonin signals darkness to the suprachiasmatic nucleus, promoting sleep onset. DSIP promotes delta-wave activity in the cortex, supporting sleep depth and restoration. They address different aspects of sleep, through different pathways, with different clinical implications.
The conflation of "falling asleep" with "sleeping well" — in both public understanding and commercial product development — may be the single most significant reason that DSIP remained in research laboratories while melatonin filled pharmacy shelves.
Emerging relevance
Recent advances in peptide synthesis, oral delivery systems, and consumer awareness of sleep architecture have renewed interest in DSIP as a supplemental compound. Several companies have begun offering oral DSIP formulations, making the peptide accessible outside clinical settings for the first time in its 50-year history.

Oral DSIP supplementation. Advances in peptide encapsulation have enabled delivery of bioidentical DSIP in capsule form, addressing the bioavailability limitations that constrained earlier research to intravenous administration.
The growing body of consumer interest coincides with a broader shift in sleep science — away from the binary question of consciousness ("are you asleep or awake?") and toward the more nuanced question of sleep architecture ("is your sleep doing its job?").
Deep sleep — the delta-wave phase that DSIP specifically targets — is increasingly recognised as the foundation of overnight recovery. Growth hormone release, cortisol regulation, tissue repair, immune function, and glymphatic brain waste clearance all occur preferentially during slow-wave sleep11. Age-related decline in deep sleep duration has been linked to accelerated cognitive decline, increased cardiovascular risk, and impaired metabolic function12.
The recognition that deep sleep declines progressively with age — and that this decline is driven in part by reduced endogenous peptide signalling — positions DSIP not merely as a sleep aid but as a potential intervention in the broader biology of ageing.
Whether the next 50 years of DSIP research will match the scientific promise of the first remains to be seen. What is clear is that the question Schoenenberger and Monnier asked in a Basel laboratory in 1974 — what is the chemical basis of deep sleep? — has never been more relevant.

From Basel to the bedside. Fifty years after its discovery in a Swiss laboratory, DSIP is entering the consumer supplement market for the first time — raising the prospect that the peptide's clinical promise may finally reach the people it was shown to help.
References
Monnier, M., Dudler, L., Gächter, R., Maier, P.F., Tobler, H.J. & Schoenenberger, G.A. The delta sleep inducing peptide (DSIP): Comparative properties of the original and synthetic nonapeptide. Experientia 33, 548–552 (1977).
Schoenenberger, G.A. & Monnier, M. Characterization of a delta-electroencephalogram sleep-inducing peptide. Proc. Natl Acad. Sci. USA 74, 1282–1286 (1977).
Graf, M.V. & Kastin, A.J. Delta-sleep-inducing peptide (DSIP): a review. Neurosci. Biobehav. Rev. 8, 83–93 (1984).
Graf, M.V. & Kastin, A.J. Delta-sleep-inducing peptide (DSIP): an update. Peptides 7, 1165–1187 (1986).
Reference to DSIP in human breast milk — primary source to be confirmed.
Schoenenberger, G.A. Characterization, properties and multisite functions of delta-sleep-inducing peptide (DSIP). Pharmacol. Ther. 2, 1–29 (1984).
Schneider-Helmert, D., Gnirss, F., Monnier, M., Schenker, J. & Schoenenberger, G.A. Acute and delayed effects of DSIP (delta sleep-inducing peptide) on human sleep behavior. Int. J. Clin. Pharmacol. Ther. Toxicol. 19, 341–345 (1981).
Schneider-Helmert, D. DSIP in insomnia. Eur. Neurol. 23, 358–363 (1984).
Clinical pharmacology reference for trazodone side-effect profile and long-term use patterns.
Brunner, D.P., Dijk, D.J., Münch, M. & Borbély, A.A. Effect of zolpidem on sleep and sleep EEG spectra in healthy young men. Psychopharmacology 104, 1–5 (1991).
Xie, L. et al. Sleep drives metabolite clearance from the adult brain. Science 342, 373–377 (2013).
Mander, B.A., Winer, J.R. & Walker, M.P. Sleep and human aging. Neuron 94, 19–36 (2017).
This article is a research review prepared for educational purposes. It does not represent a publication of Nature or any peer-reviewed journal. Statements about DSIP have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.